Science at the authorities – deceptive and fraudulent!

FDA /CDER often conducts workshops guiding the industry to assist in drug development approaches so that the approval of their drug applications goes smoothly and expeditiously.
A recent example of such a workshop is “Advancing Generic Drug Development, Translating Science to Approval” (link).
This workshop is to help the industry and small businesses whose sole business is manufacturing drug products by the “experts” at FDA who never manufacture any drug product.
So how does it make sense? It does not! Therefore, understandably, FDA and worldwide authorities make bizarre and glaringly stupid mistakes in “guiding” and “helping” the industry.
The workshop title, “Advancing Generic Drug Development,” is scientifically incorrect because there cannot be a “generic drug.” Generics are always “drug products.” For example, acetaminophen is a drug (a pure chemical compound). However, Tylenol is a product, a composite of chemicals, including acetaminophen. Different manufacturers can manufacture acetaminophen products, but they all must have the same drug (acetaminophen).
However, for some mysterious reasons, in fact, in ignorance, medical and pharmaceutical experts do not see this difference. Scientifically, manufacturing both (drug and drug products) is a part of the chemical industry. In most cases, drugs can be purchased from chemical manufacturers or distributors with the same or better quality attributes as required by the FDA or local or national
authorities.
However, drug products, even though they are composite of chemicals, often thoroughly investigated, and are manufactured based on chemistry principles and methods, cannot be purchased from chemical manufacturers. This is because authorities prohibit the chemical industry from selling. Instead, they can only be obtained from still chemical manufacturers but approved by the
authorities, which label them pharmaceutical manufacturers.
In short, a pharmaceutical manufacturer is a chemical manufacturer. The labeling and approval of pharmaceutical manufacturing are done by authorities dominated by experts, mainly physicians and pharmacists. Therefore, a chemical manufacturing plant becomes a pharmaceutical plant by getting “approval” from physicians and pharmacists.
I hope people see here the anomaly that physicians and pharmacists are guiding the development and manufacturing of chemical products. However, these professionals do not study or are trained in the chemistry/science aspect of these products/pharmaceuticals.
Instead, they are trained to suggest (use orprescribe) and administer the pharmaceuticals. They are the users of chemical compounds and products. Please consider studying the curriculum of medical and pharmacy degree programs.
It is like a chef uses farm products to prepare dishes. A chef uses and knows about vegetables, meat, and dairy items but is not expert or knowledgeable in producing (“manufacturing”) the farms’ items, let alone guiding the farmers on how to create/develop the farm items.
On the other hand, modern-day physicians and pharmacists (chemical users) are considered and promoted as experts in chemical development and manufacturing, mainly by health authorities and news media around the world The even more bizarre thing is that these medical and pharmacy experts are also promoted as scientists when, in reality, they never have studied or trained in science or conducted relevant scientific experimentation.
Please consider looking at any curriculum for such degree programs (e.g., link) Now let’s consider the topics discussed during the workshop (link).
“TOPICS COVERED
- Peptide and ligonucleotide Active Pharmaceutical Ingredient (API) Sameness and Impurity Assessment Considerations
- Drug-Device Combination Products
- Long-Acting Injectables
- Oral Complex Drug Products
- Nasally Administered Products
- Quantitative Methods and Model-Integrated Bioequivalence Approaches
- Suitability Petitions”
Technically and scientifically, most, if not all, relate to testing the drug products, not the drug development, as noted in the workshop title, i.e., testing chemical compounds/products. Testing is conducted following (FDA and other similar regulatory authorities) in-house developed protocols called guidelines or guidance documents.
From a medical products perspective, the two most common testing approaches are: (1) in vitro or drug dissolution testing and; (2) In vivo or bioequivalence (BE) testing. BE testing is sometimes referred to as clinical testing or trials.
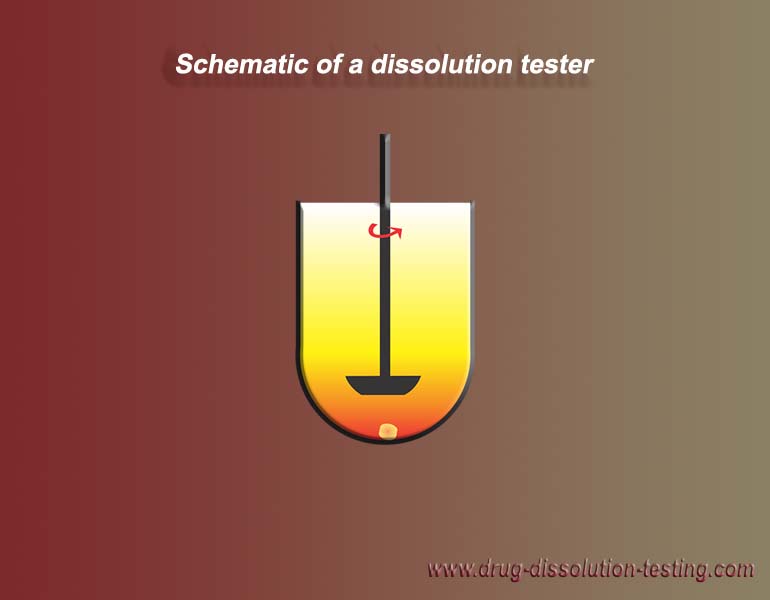
In vitro or drug dissolution testing is based on measuring drug release from its product within a round-shaped beaker with a stirrer called a drug dissolution tester or apparatus (see here). It is a well-established regulatory requirement for a drug product to be approved for marketing. A more detailed description of the technique, its scientific basis, and its applications may be found here (link).
{kind=link}
However, unfortunately, the technique has not been validated (authenticated) for its use, i.e., it has not been shown that the technique or tester can produce relevant and valid dissolution results. In fact, considering the physical limitations of the testers, they cannot provide valid and relevant results (link).
In a recent response to the Citizen Petition for withdrawing the use of the non-validated dissolution testers, while acknowledging the invalidity of the testers, FDA rejected the petition describing that the tester becomes validated when one tests the products following in-house developed guidelines (link). Note the in-house developed guidelines are based on these invalid testers.
A test product (a product under development) cannot be used to validate a test. Using a test product to validate the tester is illogical and unscientific. It confirms that experts have no idea of the fundamental principles and requirements of science, establishing that experts at the FDA cannot be considered scientists.
In scientific terms and following FDA’s cGMP (Current Good Manufacturing Practices) Guidelines, using invalid tests or testers is considered a deceptive practice punishable by law and its own (FDA) rules and guidelines (link). However, FDA arrogantly enforces the guidelines as science-based. No one would make such a claim or enforce such a policy if they had studied science to any degree.
Therefore, all claims by the FDA and other regulatory authorities about the product assessments must be considered false and fraudulent. On the other hand, FDA and regulatory
agencies, particularly in developed countries, defend their product assessment and approval claims based on the second test, the BE test.
First, this test is not conducted on products that consumers/patients use, i.e., commercial batches or lots. Therefore, the test has no direct relevance for consumers or patients. The test is only conducted on test products to get regulatory approval. Commercial products are only tested using the above-mentioned invalid drug dissolution test. Like the drug dissolution, the BE test has not been validated or authenticated, i.e., the validation for its intended purpose.
BE test monitors the release of a drug from its product in human subjects, unlike the dissolution test, which monitors the same characteristic in a round bottom beaker. n a BE test, 18-24 subjects are administered two different (test and reference) drug products (such as tablets or capsules). Following the administration, blood samples are withdrawn from the subjects to measure the blood drug levels, which indicate drug release in the body or the GI tract.
If the blood levels from both products are similar, with acceptable variability or variance, then the products are considered BE. It means both products are presumed to have the same therapeutic effect. This forms the basis of generic product development. i.e., showing a generic product (test) is equivalent to its branded (reference) version. The question is, does this test monitors the sameness in the drug release of the test and reference products?
That is, has this test been validated for this purpose? The answer is no. Such validation requires products having known and established drug release characteristics.
However, no such reference standards or products exist. So in current practices, comparative studies are conducted with brand-name and generic products. If the drug release comes out within
80 to 120 percent of the branded, the generic is declared acceptable and promoted as a high-quality product with a science-based assessment. This acceptable difference in drug release
within the 80 to 120 percent range is an arbitrary standard.
It assumes that if the difference is 20 percent lower or higher than the reference product, the body would not recognize such a difference and will consider the product as the
same or equivalent.
The troubling part is that 80 to 120 percent difference is assumed to be because of the products, but in reality, it is the physiological difference in body drug absorption mechanism, i.e., bringing
a drug from the GI tract to the bloodstream (link). The product has no contribution to this variability. So it means the BE testing does not assess product characteristics but the body’s
physiological variability.
In fact, the physiological variability could be even higher depending on the subjects’ or study requirements, such as testing with or without a meal. The point is that the test has higher variability than expected for the tested item.
How could such a test be allowed? Medical and pharmacy-dominant experts are not aware of this flaw. It is a blatant reflection of a lack of competency or ignorance of science, particularly the science of testing or analytical chemistry. This is a fundamental principle of the analytical testing which is being violated. So, experts and authorities are not following science in developing or assessing drug products.
Hence, they are teaching or guiding the industry with false science. Therefore, the drug products one obtains cannot be claimed to have the desired and scientifically valid attributes.
As a side note, the current COVID-19 pandemic is monitored with in-house (CDC) developed tests, known as PCR or Antigen.
Unfortunately, these tests are also not validated because, for validation, one requires reference standards of the virus, its RNA, or spike protein, which are missing as well. Without validation, a test cannot tell anything, hence the fakeness or fraud of the virus and its pandemic (link).
The practice of using invalid tests is ingrained in the regulatory system. It reflects the ignorance and incompetence of the science at the regulatory authorities. One may ask how and why such a fraudulent practice has not been caught and addressed.
The reason is that the system is controlled and managed by a peer-review system. No independent third-party review or audit is allowed. Opinions by third parties are considered irrelevant and/or conspiracy theories, as reflected by the censoring of often valid scientific questions and thoughts.
An urgent audit of the so-called science practices within the regulatory authorities is urgently needed. In the meantime, any claim referencing science by medical and pharmacy professionals concerning creating medicinal products should be put on hold.
To conclude:
1. The guidance the authorities and experts provide on product development and assessment is based on false and fraudulent science.
2. An urgent audit by an independent third party, not peers, is needed to stop the fake science practice.
See more here drug-dissolution-testing
Please Donate Below To Support Our Ongoing Work To Defend The Scientific Method
PRINCIPIA SCIENTIFIC INTERNATIONAL, legally registered in the UK as a company ![]() incorporated for charitable purposes. Head Office: 27 Old Gloucester Street, London WC1N 3AX.
incorporated for charitable purposes. Head Office: 27 Old Gloucester Street, London WC1N 3AX.
Trackback from your site.
Wilson Sy
| #
The FDA is just a trade guild for Big Pharma masquerading as regulator.
Reply
Jerry Krause
| #
Hi Saeed,
Not sure what prompted this pondering, but you seemed to be the best person to share it and possibly receive a response from someone whose experience, therefore knowledge, I trust.
“Bruce Ames, (born December 16, 1928, New York City, New York, U.S.), American biochemist and geneticist who developed the Ames test for chemical mutagens. The test, introduced in the 1970s, assessed the ability of chemicals to induce mutations in the bacterium Salmonella typhimurium. Because of its sensitivity to carcinogenic (cancer-causing) human-made substances, which led to bans on the commercial use of several synthetic chemicals, the test made Ames a hero to environmentalists. However, he later changed his position on synthetic chemicals, following the realization that many naturally occurring substances are also carcinogenic. As a result, during the late 1980s and the 1990s, he came into conflict with environmentalists who had hailed him as an asset to their cause. Ames devoted much of his career to the study of cancer and aging, summarizing his research in more than 500 publications.” (https://www.britannica.com/biography/Bruce-Ames)
It was very difficult to find this what I knew (because I was living and reading during from 1980 t0 2000) was a historical fact about Bruce Ames and his Ames test.
However, even “Britannica” tries to rewrite history. “However, he later changed his position on synthetic chemicals, following the realization that many naturally occurring substances are also carcinogenic.” Fact: BENZENE is not a synthetic chemical. And Ames knew his test only proved the ability of certain chemicals to cause mutations. And in the case of “many naturally occurring substances”, some of these substances were foods whose many naturally occurring chemicals were never isolated and tested to see which NATURAL MOLECULES, of many in a common food, might be causing a causing a mutation according to his test.
But, any one who writes for “Britannica” is an AUTHORITY with more knowledgable than you or I, who likely have many more years of experience the “Britannica” authority.
Have a good day, Jerry
Reply
Saeed Qureshi
| #
Hi Jerry:
Thanks for your comment.
I know about the Ames test. However, not in greater detail. I think your question/pondering is about my view in the above article, i.e., “The practice of using invalid tests is ingrained in the regulatory system.”
Like PCR, the Ames test is developed in the biological area. Biological tests (often referred to as bioassays to sound flashy and modern) are still standard tests, so they must follow standard test requirements, i.e., test validation. Unfortunately, most of them are not validated in the true sense of the meaning of “validation,” including the Ames test. I stand to be corrected here.
Therefore, the Ames test should also give false outcomes like the PCR or Antigen tests, which you described, getting mutagenicity outcomes with natural and non-natural source chemicals.
I am starting to doubt the relevancy and accuracy of all the tests in the medical area, including cancer. It appears they are all designed to provide desired results on demand! God help us with this “science.”
Reply
Jerry Krause
| #
Hi Saeed,
Thank you for your comment. You wrote “I am starting to doubt the relevancy and accuracy of all the tests in the medical area, including cancer. It appears they are all designed to provide desired results on demand! God help us with this “science.” “ This reminded me of some history of science and a generally common quote. “Those who don’t know history are destined to repeat it.” (Irish statesman Edmund Burke”
Galileo, with his telescope observations proved that the Earth did not standstill and that it rotated about axis as it revolved about the sun. But his observations were ‘qualitative’ and not quantitative as these of Tycho Brahe’s were. A historical fact is that in the ‘beginning’Galileo, Tycho, Kepler “believed” the shape of the planets’ orbits about the Sun were perfect circles. But when Kepler could not fit Tycho’s measurements to a circular path, Kepler discovered that an elliptical path gave a better fit to Tycho’s data. And I read that Galileo reasoned, that since his Creator God was perfect and a circle was perfect, and we know he refused to accept the valid its of Brahe’s data and Kepler’s mathematical analysis of the data.
Should we consider that Galileo was EVIL? I certainly do not.
Next, I move to the later case of Ptolemy, another astronomer, who believed that the planets orbited the Sun but the Earth, from where he made his observations, was still the center of the universe. However, Ptolemy observed that sometimes the motion some planets reversed their direction of revolution about the SUN when viewed against a background of ‘fixed’ stars. Which observation made no sense. But he “believed” that the Earth was the center of the universe and would not give up his belief.
Should we consider that Ptolemy was Evil? I certainly do not and I consider because his stubbornness Copernicus saw that Ptolemy data pointed to the idea that the Sun was the center of our solar system.
Hence, have Faith, because the lack of medical understanding is getting SO BAD people might begin to question it and sort out what might true and what is absolutely wrong.
However, I do not know the future and I leave it to my Creator God to judge who is good and who is evil. For I know I know I have made many mistakes during my lifetime and will continue to make more mistakes.
Have a good day, Jerry
Reply